It remains for you to prove that there are no veins in a deltoid muscle, ever, despite what it says in the nurses' book. You can't, because it's not true.
I already showed the image. Here are some more. As I said, so long as the needle is not so long that it can pass through the muscle into the veins, there is no risk.
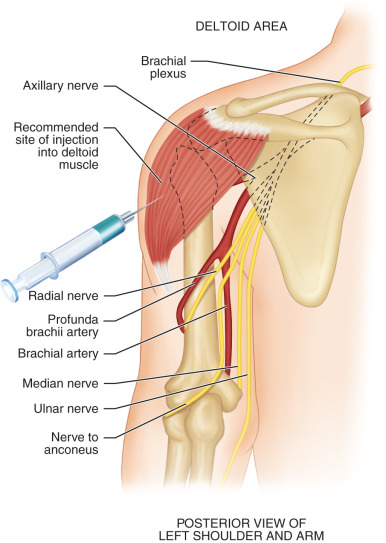
This one even has a needle shown, it shows nerves too (which the puncturing of is likely to cause more problems then veins)
This is a good detailed one of the veins - note, none in the lump of muscle used for injections
Maybe this is Grays? Certainly similar style. Again, big muscle, no veins in the injection zone
As I said before - this is
WHY intramuscular injections are given in the deltoid. It's because it is so hard to hit a vein.
More injections used to be given in the buttocks, (there's a big nerve which if hit can paralyse - I nurse told me that, just before injecting by buttock once!) but this is probably only needed if your muscle mass in your arm is very low - maybe why I had one as a child.
Anyway, if there are untrained people out there giving vaccines, I stand corrected. In Essex, their training was top notch, judging by how good at it they were.
For every person giving the vaccine, there was an admin person doing all the paperwork (computer) - maybe in some NHS locations they do it differently, with everybody trying to do everything? I really don't know, I have not see any vaccination centres other than the ones in Essex I have been to.
As for ...
I daresay you or I could jab someone with a few minutes' demo.
These are the requirements:
"Legislation allows a wider group of staff to undertake training to deliver vaccines. This includes many
allied health professionals, healthcare scientists and
dental staff, as well as other individuals
with appropriate first aid training, who are
able to undertake additional comprehensive training; so opportunities for flexible, paid roles are open to a huge variety of people."
https://www.england.nhs.uk/coronavirus/join-the-nhs-covid-19-vaccine-team/
That does not sound "untrained" with a "few minutes demo" to me.
Maybe your vaccinator was just teasing.